Table of Content
Used for urination and sexual intercourse, the penis is made up of two erectile cylinders that enlarge with blood during erection. A tough fibrous, partially elastic outer casing surrounds the cavernosa. The corpus spongiosum surrounds the urethra , a tube that runs from the bladder to the end of the penis. If you have had an erection that has lasted more than two hours, you should go to the nearest emergency department for medical attention.
Treating priapism quickly reduces the risk of permanent problems getting and keeping erections. Priapism is an erection of the penis that lasts for more than 4 hours without physical and mental stimulation. It develops when blood becomes trapped in the penis and is unable to drain. A common cause of nonischemic priapism is trauma or injury to your penis, pelvis, or the region between the base of the penis and the anus .
Intermittent (stuttering) priapism
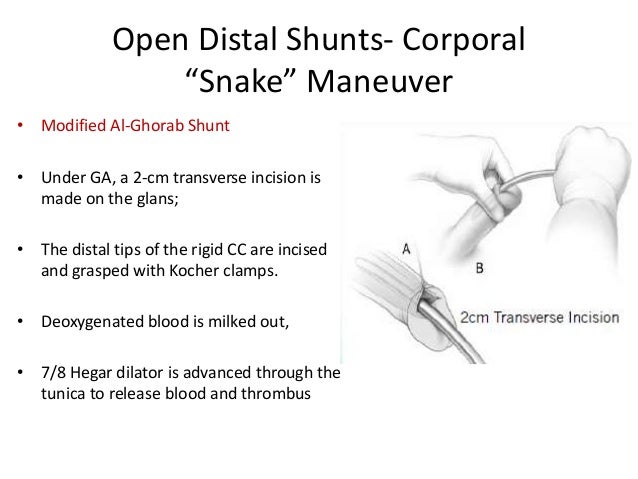
Surgery might also be necessary to repair arteries or tissue damage resulting from an injury. If other treatments aren’t successful, a surgeon might perform surgery to reroute blood flow so that blood can move through your penis normally. Your blood can be tested to measure the number of red blood cells and platelets present. Results might show evidence of diseases, such as sickle cell anemia, other blood disorders or certain cancers. The condition may occur in any age group, but most common occurs at years of age in those with sickle cell disease induced priapism.
Where the latter is not available, further conservative management should be conducted or the patient should be directed to a facility which has an interventional vascular radiologist who is experienced in this form of intervention. For patients with persistent NIP who have failed a period of observation and are bothered by persistent penile tumescence, and who wish to be treated, first line therapy should be percutaneous fistula embolization. One factor which may be used to determine whether intervention is appropriate is the extent of penile rigidity. As an example, a mild erection (i.e., not sufficient to penetrate without assistance) would not require treatment, whereas a fully rigid erection might, depending on other factors.
Prolonged Erection Following Intracavernosal Vasoactive Medication
Furthermore, in cases where studies show conflicting evidence or evidence is sparse, panelists may still use clinical judgment to inform a guideline statement. Note that the worst possible rating for RCTs is Level B. Therefore, evidence comprised of RCTs and systematic reviews that included only RCTs would be judged as either Level A or Level B. Since the last American Urological Association priapism guideline,3 several other additions have been made to address various diagnostic modalities.
The key differentiating factor between the current definition of recurrent ischemic priapism and other recurrent priapism-like conditions is the requirement of confirmed penile ischemia. Decisions regarding placement of a penile prosthesis in a patient with acute ischemic priapism must be made after weighing multiple factors. These include, but are not limited to, the quality of the history provided relative to duration of persistent priapism, overall condition of the patient, health literacy and comprehension, and physician experience. Perhaps due to the complex nature of such decision-making, there are no RCTs relevant to this pathway. The Panel felt that it was important to highlight a clinician’s responsibility in managing office-based erectogenic therapies.
What are the home remedies for priapism?
In rare cases, priapism may be related to cancers that can affect the penis and prevent the outflow of blood. Insights of priapism mechanism and rationale treatment for recurrent priapism. Make a list of all medications, vitamins, herbs and supplements that you're taking. Your doctor might order a blood or urine test to screen for drugs that might be the cause of priapism. Well, finally we have come to conclusion where we have come to know about Priapism and its home remedy treatment.

In the majority of cases presently acutely to the emergency department, a corporal blood gas should be obtained during the initial evaluation to diagnose the priapism subtype. However, there are certain clinical situations where a blood gas may be omitted at the clinician’s discretion. Examples include priapism induced by in-office or at home ICI therapies, cases of recurrent ischemic priapism (i.e., SCD), or when the diagnosis is abundantly clear by history and examination alone. Criteria for inclusion and exclusion of studies was based on the Key Questions and the populations, interventions, comparators, outcomes, timing, and study designs of interest. Populations were male patients of any age with priapism secondary to sickle cell disease, with NIP, or with stuttering priapism; or adult males with a priapism episode following ICI. Stuttering priapism was defined as recurrent episodes Eligible study designs were RCTs, cohort studies, and case series with at least two patients.
What causes priapism?
Where gaps in the evidence existed, the Panel provides guidance in the form of Clinical Principles or Expert Opinions with consensus achieved using a modified Delphi technique if differences of opinion emerged. A Clinical Principle is a statement about a component of clinical care that is widely agreed upon by urologists or other clinicians for which there may or may not be evidence in the medical literature. Expert Opinion refers to a statement, achieved by consensus of the Panel, that is based on members' clinical training, experience, knowledge, and judgment for which there may or may not be evidence. Ideally, different key questions required different types of evidence in terms of trial design and study type. However, realizing that the evidence base for this topic would be limited, very liberal inclusion criteria was adopted. The vast majority of studies were observational in design and most of these were retrospective.
If over-the-counter and prescription treatments do not work and the erection has been present for 4 hours and/or is painful, immediately visit the ER for treatment. Priapism is an involuntary erection which lasts more than 4 hours and is unrelieved by ejaculation. It is sometimes a symptom of Penile Injection therapies, which is why anyone considering Trimix or similar injections should approach them carefully under the guidance of a physician. Surgical intervention – If the condition does not resolve with conventional therapy, surgery is the only other option available. Those blood vessels responsible for the condition are located by ultrasound and removed in surgery. Expectant approach – As the condition poses little threat to erectile function or appearance, the patient may only be observed, as the condition may resolve on its own accord.
The AUA nomenclature system explicitly links statement type to body of evidence strength, level of certainty, magnitude of benefit or risk/burdens, and the Panel’s judgment regarding the balance between benefits and risks/burdens . Strong Recommendations are directive statements that an action should (benefits outweigh risks/burdens) or should not (risks/burdens outweigh benefits) be undertaken because net benefit or net harm is substantial. Moderate Recommendations are directive statements that an action should (benefits outweigh risks/burdens) or should not (risks/burdens outweigh benefits) be undertaken because net benefit or net harm is moderate.
"So the first step in the management of ischemic priapism, as it turns out, is also the first treatment intervention, which is to try and aspirate the penis flat, get all the old blood out." The less common, nonischemic kind of priapism tends to be easier to treat than the ischemic variety, Akakpo said. Aberrant arterial blood flow has to be stopped, usually with nonsurgical radiological treatment via embolization, a procedure that aims to block blood vessels. With an injection into the penile vessel, a urologist can close the fistula, or abnormal connection, that's contributing to the abnormal passage of blood. Broderick said this phenomenon usually signals recurrent ischemic priapism. Episodes of stuttering priapism can last one to five hours, he said, but they can also continue for about 12 hours after a nocturnal erection fails to resolve itself, probably prompting an emergency room visit at that point.








No comments:
Post a Comment